
This summer Professor Gisella Kagy and I examined the impact of a Maternal and Child Health and Family Planning Program (MCH-FP) on infant mortality in Bangladesh. The MCH-FP program was started in October 1977 by the International Center for Diarrheal Disease Research in Matlab, Bangladesh. The Matlab region is a sub-district in Bangladesh, with a population of about 200,000 people, located 55 km south of Dhaka, the country’s capital.
The MCH-FP program was implemented as a randomized control trial between 1977-1988. The Matlab region was divided into a treatment and comparison area , with about half the population receiving the child health and family planning measures while the other half of Matlab only had access to these services after 1988. Some of the program services included the provision of free modern contraception, tetanus vaccinations, polio and tuberculosis immunizations, and vitamin A supplementation. These services were provided at the home of the beneficiary by local health care professionals and this door to door delivery was unique to the treatment area.
Our research question was to examine the first and second generation impacts of this program on infant mortality. So we were interested in analyzing the program impact on those infants born during the experimental period as well as the impact on their subsequent children. Our raw data consisted of individual level birth, death, and migration information from 1974 to 2012. I was able to bring this information together using Stata to produce a final data-set for our analysis that was unique by person, and contained variables indicating the treatment status of a person, whether a person lived in Matlab during the experimental period, and whether someone died.
Below are some examples of our results with brief explanations:
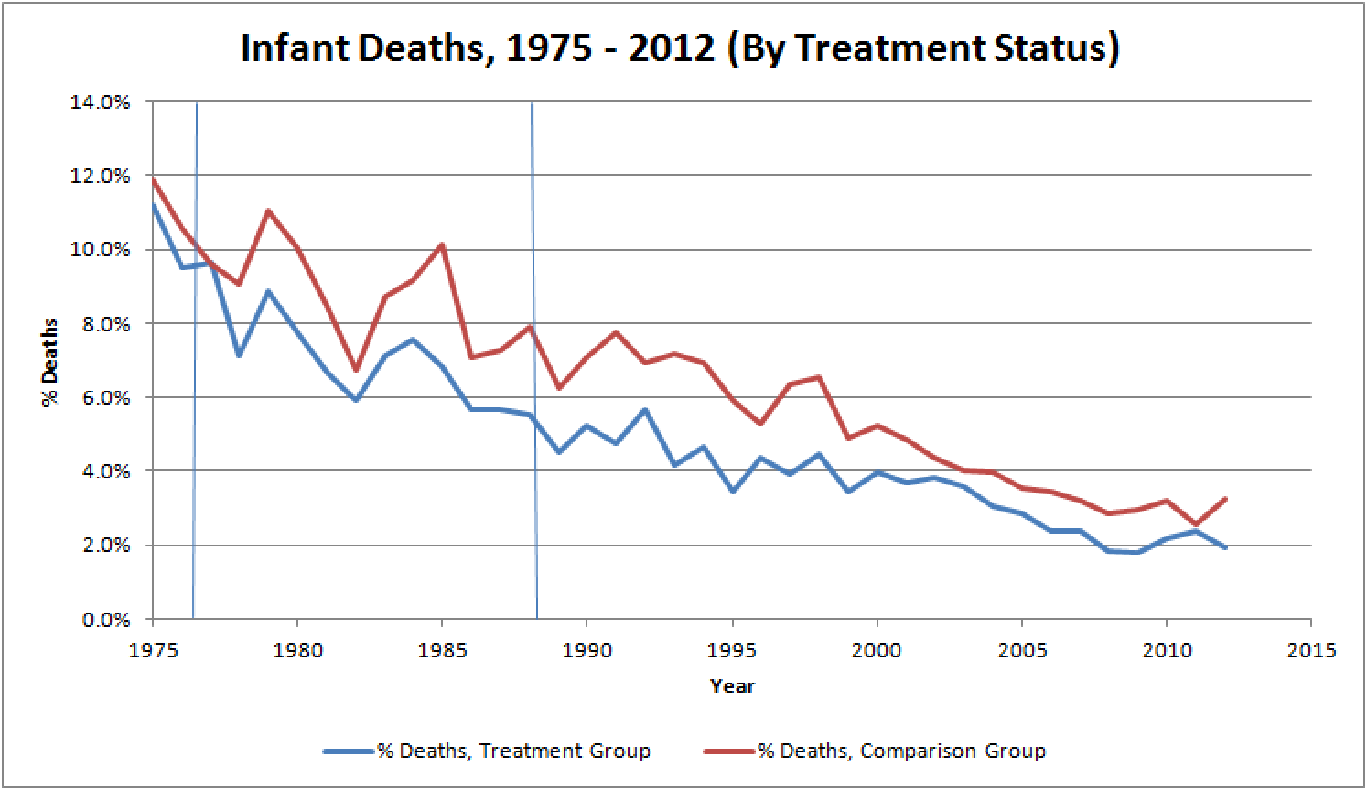
This graph shows yearly infant deaths between 1975 and 2012. We can see that when the program started in 1977, the treatment and comparison groups had a similar infant mortality rate. However immediately following the program, the infant mortality rate in the treatment area was much lower than the comparison area. This was true not only for the experimental period but we can see that these effects persisted beyond 1988, suggesting that the program also had strong inter-generational impact. These results are consistent with our econometric analysis which revealed that the program had a significant impact of reducing infant mortality by 1.2 percent in the treatment area as opposed to the comparison area once we controlled for differences in household characteristics and a person’s sex.

This graph shows the percent of deaths for 0 – 5 year olds by year for 1975 – 2012. We can see that the death rate for this age group was only slightly higher in the comparison area when the program started but this difference increased during the experimental period and persisted up till 2003 when we see the death rates converge again. Once again this demonstrates the strong inter-generational impact of this program. These results are also consistent with our econometric analysis which showed that the program reduced the under 5 death rate by 1.8 percent in the treatment area as opposed to the comparison area once we controlled for differences in household characteristics and a person’s sex.