
 Immigrants are often portrayed as free loaders who exploit and overuse American health services. Although immigrants are net contributors to the U.S. economy, the misconception remains that they are a burden to native-born taxpayers. However, a report by the University of California and the Mexican government found that recent immigrants from Mexico are half as likely to use emergency rooms as native-born whites and Mexican Americans (2005). Also, when controlled for minority groups, Latino immigrants accounted for $962 in per capita health care expenditures in 1998, compared to $1,870 for native-born Latinos. Black immigrants averaged $1,030 in health care expenditures, compared to $2,524 for native-born blacks (Mohanty et al. 2005). As many politicians call for the securing of our borders and the elimination of “magnets” for undocumented migrants, a 1996 study concludes, “there is no reputable evidence that prospective immigrants are drawn to the U.S. because of its public assistance programs” (International Migration Policy Program 1996:3).
Immigrants are often portrayed as free loaders who exploit and overuse American health services. Although immigrants are net contributors to the U.S. economy, the misconception remains that they are a burden to native-born taxpayers. However, a report by the University of California and the Mexican government found that recent immigrants from Mexico are half as likely to use emergency rooms as native-born whites and Mexican Americans (2005). Also, when controlled for minority groups, Latino immigrants accounted for $962 in per capita health care expenditures in 1998, compared to $1,870 for native-born Latinos. Black immigrants averaged $1,030 in health care expenditures, compared to $2,524 for native-born blacks (Mohanty et al. 2005). As many politicians call for the securing of our borders and the elimination of “magnets” for undocumented migrants, a 1996 study concludes, “there is no reputable evidence that prospective immigrants are drawn to the U.S. because of its public assistance programs” (International Migration Policy Program 1996:3).
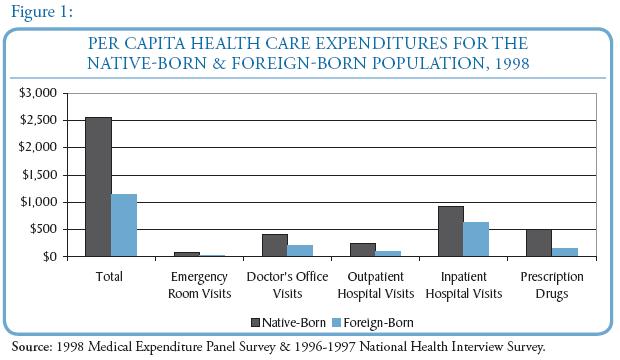
Poverty, jobs that fail to offer health insurance, immigration status, and federal and state policies that limit access to publically funded insurance all reduce health insurance coverage rates for immigrants. On average, immigrants received about $1,139 in health care, compared with $2,546 for native-born residents. Although immigrants comprised 10 percent of the U.S. population in 1998, they accounted for only 8 percent of U.S. health care costs (Mohanty et al. 2005). A significant proportion of immigrants work in low-paying jobs with small firms that do not offer health insurance. Ultimately, these immigrants do not receive quality health care and lack timely preventive services. These delays result in some immigrants attaining medical care only when they become very ill. Additionally, legislative initiatives such as the Personal Responsibility and Work Opportunity Reconciliation Act of 1996 (PRWORA) eliminated equal access to public benefits for all legal permanent residents. The PRWORA prevented states from using federal funds to provide Medicaid and State Children’s Health Insurance Program (SCHIP) coverage for most legal immigrants who have resided in the United States for less than 5 years (International Migration Policy Program 1996). By not allowing all legal permanent residents the same public benefits, the government is directly compromising the health of immigrants until they have resided in the America for 5 years or attain health insurance through employment.
Even among immigrants who meet the qualification for publicly funded health insurance, fear and confusion often create barriers to enrollment. What could be reflections of a harmful immigration process or general distrust of the American government could cause concern about becoming a “public charge,” which would make them ineligible for U.S. citizenship and could result in deportation (Berk and Schur 2001).
Interestingly, despite the legislative and social issues complicating immigrant health care, male and female immigrants had, respectively, 3.4 and 2.5 years longer life expectancy than the US-born (Singh and Miller 2004). There are many possible reasons for this statistic. First, people immigrating may be healthier than those who remain in their countries of origin, for the process is generally difficult. This form of immigrant selectivity could skew the general health of their countries of origin, but underscores the point that America is not a welfare magnet. Also, it is possible that immigrants possess more favorable health habits, such as lower rates of smoke, drinking, and better diet. Regardless of the reasons, it is crucial to realize immigrants use less public assistance than native-born citizens, but may very well be suffering at the hands of harsh legislation and lack of health insurance.
Works Cited
Berk, Marc L. and Claudia L. Schur.2001. “The Effect of Fear on Access to Care Among
Undocumented Latino Immigrants.” Journal of Immigrant Health 3(3):151-6.
International Migration Policy Program of the Carnegie Endowment for International
Peace & the Urban Institute. 1996. “Immigrants and Welfare,” Research Perspectives on Migration 1(1):1-15
Mohanty, Sarita A., Steffie Woolhandler, David U. Himmelstein, Susmita Pati, Olveen
Carrasquillo and David H. Bor. 2005. “Health Care Expenditures of Immigrants in the United States: A Nationally Representative Analysis.” American Journal of Public Health 95(8):1431-1438.
Singh, Gopal K. and Barry A. Miller. 2004. “Health Life Expectancy, and Mortality Patterns Among Immigrant Populations in the United States.” Canadian Journal of Public Health 95(3):14-21
University of California, Los Angeles Center for Health Policy Research and the National Population Council of the Government of Mexico. 2005. Mexico-United States Migration: Health Issues.